
Dental Practice Ulf Krueger-Janson
+49 69 590303
- Deutsch|
- English


 Creating a composite filling, a crown, a veneer, or a full-ceramic partial crown, fundamentally requires understanding how they will facilitate chewing
Creating a composite filling, a crown, a veneer, or a full-ceramic partial crown, fundamentally requires understanding how they will facilitate chewing
Reconstruction and Function
Functional dental prosthetics, tooth replacements, occlusion, CMD, Wax-up, and functional analysis in Frankfurt
The purpose of restorative and reconstructive dental surgery is to create teeth replacements and fillings which functionally integrate easily in the physiological chewing (or stomatognathic) system.
Analysing and modelling relevant dental structures that enable the movement of teeth to break food into smaller parts provides the information needed to restore the ability to chew.
(See under Prosthetics and Case Reports I and II in Publications –QZ 02 & 03, 2010 )
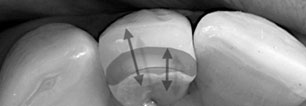
 A composite filling applied to an incisor. A functional pattern is drawn on the relevant teeth and taken into account at key points within the restoration to ensure its long-term success and stability.
A composite filling applied to an incisor. A functional pattern is drawn on the relevant teeth and taken into account at key points within the restoration to ensure its long-term success and stability.
Mechanical digestion begins in your mouth as your teeth tear and grind food into small bits and pieces you can swallow. This leaves marks on the upper and lower surfaces – the functional or operative surfaces. If you look carefully you can see which movements of the lower jaw are responsible for the occlusal impressions and abrasion facets. Such movements must be carefully taken into account when restoring teeth, so as to avoid improper stresses.
The lower jaw does not move only in one direction, but due to its surrounding musculature moves in 3 dimensions; this yields a 3 dimensional space within which movement is possible. The movement of the lower jaw (back to front, side to side and up and down) can be represented as vectors.
 The Occlusal Compass
The Occlusal Compass
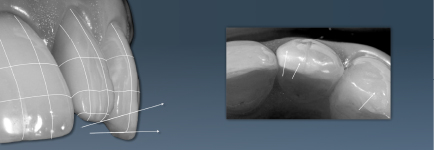
The resultant graphic is often called an “occlusal compass” (because of the arrows it contains) and is used by dentists to analyse the grinding surfaces of the teeth and to help diagnose misalignment of teeth. The way the lower jaw moves needs to be understood because chewing takes place between pairs of teeth. However, the 2 dimensional compass cannot represent the 3 dimensional movement space – because the lower jaw flexes, and the periodontal tissues also move. The method of colouring the different surfaces differently suggested by Dieter Schulz does, however, help us show how surfaces relate to movement in the lower jaw.
 Using the Occlusal Compass
Using the Occlusal Compass
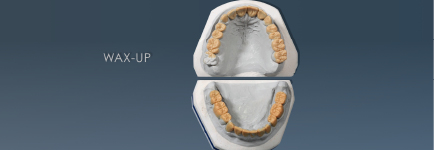
Dental technology allows a physiological reconstruction of the three-dimensional model of how teeth actually move in relation to each other, through the creation of a wax model of a “virgin” surface (the primary morphology). In addition, information from computer-supported functional analysis can be used to create a model of the movements actually made to chew food.
 Diagnostic Wax-Up
Diagnostic Wax-Up
How the upper and lower teeth relate to each other can be analysed through manipulating the two wax-ups against each other, which results in the creation of a functional, or secondary morphology. How the patient actually chews can be confirmed by using an electron microscope to analyse a plaster model. The dental technician Dieter Schulz, thanks to his energy and systematic insights, has become a leader in the use of functional reconstruction. Restoration, properly understood, is a reconstruction that enables food to be optimally chewed. He and I have often proved this to be the case!
Quote from Dieter Schulz: “The dentist and dental technician work together to restore teeth to their original functional condition. Teeth need contact with each other, not only to create stability between the two rows of teeth, but also to prepare food for digestion (created by lower jaw movement).”